The Role of Post-Op Oestrogen Therapy Explained
If you’ve recently had surgery affecting your reproductive system and walked away with a prescription for estrogen, you probably have questions. The role of post-op oestrogen therapy is genuinely nuanced. It’s not the same for every woman, every surgery, or every goal. Whether you’ve had a procedure for Asherman’s syndrome, a missed abortion, an oophorectomy, or another uterine surgery, what estrogen does for your body post-operatively depends on exactly what was removed or repaired, and what your hormones are doing as a result.
Table of Contents
- Key Takeaways
- How estrogen affects your body after reproductive surgery
- Evidence on post-operative estrogen therapy outcomes
- Personalizing your estrogen therapy after surgery
- Common misconceptions about post-op estrogen therapy
- My honest take on estrogen after reproductive surgery
- Your recovery doesn’t have to be a guessing game
- FAQ
Key Takeaways
| Point | Details |
|---|---|
| Estrogen supports tissue repair | Post-op estrogen promotes endometrial regrowth and reduces adhesion formation after uterine procedures. |
| Route of administration matters | Transdermal estrogen offers better adherence and lower clotting risk compared to oral estrogen. |
| Progestin is not always required | Women without a uterus use estrogen alone; those with an intact uterus need progestin added for safety. |
| Benefits are surgery-specific | Goals differ between endometrial recovery after missed abortion and hormone replacement after surgical menopause. |
| Risk screening is non-negotiable | History of blood clots, stroke, or estrogen-sensitive cancer changes whether systemic estrogen is appropriate. |
How estrogen affects your body after reproductive surgery
Estrogen is not just a reproductive hormone. It actively maintains the health of the uterine lining, pelvic floor muscles, vaginal tissue, and the vascular system that supplies all of them. When surgery disrupts or removes the organs that produce or respond to estrogen, the downstream effects show up faster than most women expect.
After procedures like oophorectomy (removal of one or both ovaries), estrogen deficiency causes pelvic floor muscle atrophy within weeks. That’s not a slow, gradual decline. It’s a measurable structural change in the tissue that supports your bladder, uterus, and bowel. And that matters a great deal if you want to maintain function, comfort, or fertility going forward.
For women who’ve had uterine procedures, the picture is slightly different but equally important. Surgeries like hysteroscopic adhesiolysis (for Asherman’s syndrome) or uterine evacuation after missed abortion leave the endometrial lining vulnerable. Estrogen is the key signal that tells the uterine lining to grow, thicken, and vascularize. Without adequate estrogen signaling post-surgery, the lining may fail to recover properly.
The role of hormones after surgery goes beyond replacing what was lost. Estrogen actively instructs tissue to regenerate, form new blood vessels, and resist the kind of scarring that makes future implantation or menstruation difficult.
Here’s what estrogen deficiency post-op can look like in practice:
- Thin, non-responsive endometrium that doesn’t build up before a period or embryo transfer
- Increased risk of intrauterine adhesion reformation after scar tissue removal
- Vaginal dryness and discomfort that appears sooner than expected
- Pelvic floor weakness that affects bladder control and sexual function
- Hot flashes and mood shifts following surgically induced menopause
Understanding these effects isn’t just academic. It tells you why your doctor prescribed estrogen, and what they’re hoping it will do.
Evidence on post-operative estrogen therapy outcomes
The clinical evidence on post-operative estrogen use is strongest in the context of missed abortion surgery and Asherman’s syndrome treatment. And the data is worth knowing.
A key study found that both oral and transdermal estrogen significantly improved endometrial thickness and reduced menstrual flow abnormalities compared to no estrogen after missed abortion surgery. Women who received no estrogen had thinner linings and more pronounced menstrual disruption at follow-up. This isn’t a marginal difference. It’s the kind of gap that affects whether a woman can carry a pregnancy.
The same research found that estrogen stimulates epithelial proliferation and angiogenesis after uterine surgery. In plain terms, it tells the uterine lining to grow new cells and form new blood vessels, both of which are necessary for a healthy period and for embryo implantation. It also reduces the inflammatory environment that allows adhesions to reform.
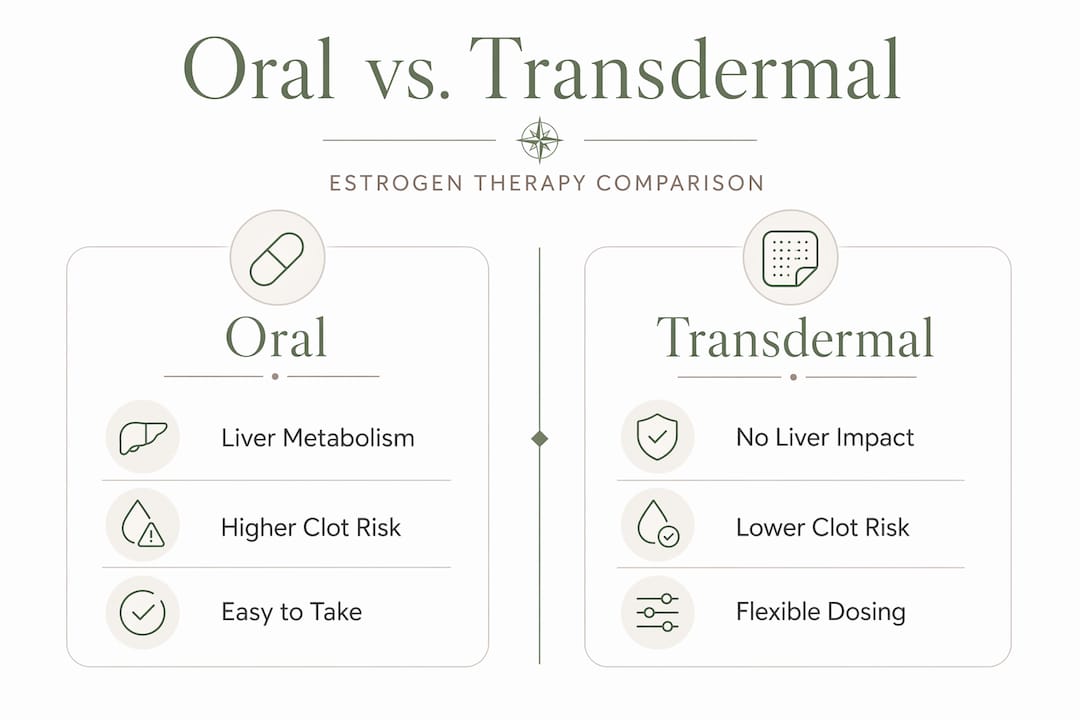
Oral vs. transdermal: what the data actually shows
| Factor | Oral Estrogen | Transdermal Estrogen |
|---|---|---|
| Endometrial recovery | Effective | Effective |
| Adherence rate | ~46.7% | ~68.3% |
| Side effect profile | Higher breast tenderness, nausea | Fewer systemic symptoms |
| VTE (clotting) risk | Higher | Lower |
| Liver metabolism | Yes (first-pass) | Bypassed |
| Best suited for | Women without clotting risk | Women with VTE risk factors |
The adherence gap between transdermal and oral estrogen is significant. If nearly half of women on oral estrogen are not completing their regimen, the recovery outcomes in that group will be compromised regardless of how effective the drug is in theory. Adherence is part of the clinical picture.
On fertility specifically, women treated with estrogen post-surgery showed higher pregnancy rates at one-year follow-up, particularly in the transdermal group. That’s a meaningful outcome for the many women reading this who are trying to conceive after a uterine procedure.
Pro Tip: If you’re choosing between estrogen routes and your doctor says both are equivalent, ask specifically about your VTE risk and whether transdermal might offer better adherence for your lifestyle. The clinical outcomes favor consistency above all else.
Personalizing your estrogen therapy after surgery
The role of post-op oestrogen therapy is not one-size-fits-all, and this is where many women get confused, especially after receiving brief post-op instructions and a prescription with minimal explanation.
The single most important factor shaping your estrogen regimen is whether your uterus is intact. Progestin must be added to systemic estrogen therapy if you still have your uterus. Estrogen alone, taken systemically over time, can cause the uterine lining to thicken abnormally and increase the risk of endometrial cancer. Progestin balances this. Women who’ve had a hysterectomy do not face this risk and use estrogen alone.
The type of progestin also matters. Micronized progesterone may carry a lower breast cancer risk compared to synthetic progestins when combined with estrogen. This is a detail worth discussing with your specialist, especially if breast cancer is in your family history.
Routes of estrogen delivery and why they’re not interchangeable
Transdermal estrogen (patches, gels, sprays) bypasses the liver entirely. This matters because transdermal estrogen generates steadier plasma levels and avoids the first-pass liver metabolism that amplifies clotting factor production. For women with a history of blood clots or cardiovascular risk, this route is significantly safer.
Vaginal estrogen sits in its own category. It works locally with minimal systemic absorption, making it a low-risk option for women experiencing urogenital symptoms like dryness, discomfort, or recurrent urinary tract infections after surgery. It doesn’t require progestin to be added and is often appropriate for women who cannot or prefer not to use systemic therapy.
Before starting any estrogen regimen, your provider should screen for these contraindications:
- Personal or family history of venous thromboembolism (blood clots)
- History of stroke or cardiovascular disease
- Estrogen-sensitive cancers (breast, uterine, ovarian)
- Active liver disease
- Unexplained vaginal bleeding
The evidence supports that systemic hormone therapy benefits outweigh risks in women under 60 without contraindications. But “no contraindications” only holds if someone actually checks. You should be asked these questions before a prescription is written. For more on how patient history shapes these therapy decisions, the post-surgical hormonal support guide at Theashermanscompass is worth reading.
Common misconceptions about post-op estrogen therapy
One of the most persistent misconceptions is that estrogen therapy is simply hormone replacement, something you take to feel normal again. After reproductive surgery, estrogen is a therapeutic tool with a specific job. That framing changes how you approach the protocol.
Here’s what often goes wrong, and how to handle it better:
-
Assuming all forms are equivalent. Oral and transdermal estrogen produce different plasma level patterns, different risk profiles, and different adherence outcomes. The estrogen therapy regimen must be matched to your surgical anatomy and your risk factors, not assigned by default.
-
Stopping early because symptoms resolve. Endometrial recovery protocols track lining thickness over multiple time points for up to a year. Feeling better is not the same as having a fully recovered endometrium. Stopping therapy before the recommended window can undo the progress.
-
Not knowing what you’re treating. The impact of estrogen post-op differs significantly between someone recovering from missed abortion surgery and someone managing surgical menopause. The goals, dosing, and duration are all different. Ask your doctor to name the specific goal for your prescription.
-
Dismissing side effects as inevitable. Breast tenderness and nausea are more common with oral estrogen. If those side effects are reducing your adherence, switching routes is a legitimate conversation, not a complaint.
Pro Tip: Keep a simple symptom log during the first four to six weeks on estrogen therapy. Note energy, sleep, mood, and any physical discomfort. This gives your doctor real data rather than a vague sense of how things are going, and it often speeds up dose adjustments.
For women who’ve had hysteroscopic surgery specifically, the hysteroscopy recovery article at Theashermanscompass covers what to expect from estrogen in the weeks after your procedure.
If conception is your goal, evidence-based information on fertility after reproductive surgery can also help you think through timing and next steps alongside your estrogen protocol.
My honest take on estrogen after reproductive surgery
I’ve spent years talking to women about what happens after surgery, and here’s what I’ve come to believe: most of us leave our post-op appointments with a prescription and not nearly enough context.
The role of post-op oestrogen therapy gets reduced to “this will help your lining.” But what that actually means, how long it takes, what you’re watching for, and when it’s working are rarely explained. That gap is where confusion, non-adherence, and unnecessary anxiety live.
What I’ve learned is that estrogen after reproductive surgery is most powerful when you understand its specific job in your specific situation. Someone recovering from adhesion removal needs to know that estrogen is actively preventing scar tissue from reforming. Someone in surgical menopause needs to understand they’re replacing a hormone their body depended on for decades, and that cutting it off abruptly has consequences that go well beyond hot flashes.
I also think we underestimate the importance of route. The data on adherence is striking. Nearly half of women on oral estrogen don’t complete their course, and I suspect a lot of that comes down to side effects that nobody warned them about. Transdermal is not perfect for everyone, but it’s worth a proper conversation rather than a default prescription.
Finally, I believe women in their 30s and 40s are often undertreated because providers apply the caution designed for older women to younger patients. The evidence is clear that benefits outweigh risks in younger women without contraindications. You are allowed to push for adequate treatment. You are allowed to ask whether the regimen you’re on is actually appropriate for your age, your surgery, and your goals.
— Daniella
Your recovery doesn’t have to be a guessing game
Navigating estrogen therapy after surgery is hard when the information you’re given is incomplete. Theashermanscompass was built for exactly this moment, when you’ve had a procedure, you have a prescription, and you need more than a pamphlet to understand what comes next.
The Complete Recovery Guide at Theashermanscompass covers hormonal therapy in the context of Asherman’s, post-D&C recovery, and uterine health from a place of genuine experience, not clinical distance. You’ll find question scripts you can take into your next appointment, a global specialist directory, and a self-care protocol grounded in the research women actually need. Ten percent of every sale funds specialist care for women who can’t access it on their own.
FAQ
What is the role of post-op oestrogen therapy?
Post-op oestrogen therapy supports tissue repair, promotes endometrial regrowth, and reduces the risk of adhesion reformation after reproductive surgeries. Its specific role depends on the type of surgery and the hormonal changes that resulted from it.
Do you always need progestin with post-op estrogen?
Not always. Women who have had a hysterectomy use estrogen alone. Women with an intact uterus must add progestin to protect the uterine lining from abnormal thickening and cancer risk.
Is transdermal estrogen safer than oral after surgery?
Transdermal estrogen carries a lower risk of blood clots than oral estrogen because it bypasses liver metabolism and produces steadier hormone levels. It also tends to have better adherence due to fewer systemic side effects.
How long does post-operative estrogen therapy last?
Duration varies by surgery type and goal. Endometrial recovery protocols after uterine procedures typically run for several months, with lining thickness tracked at multiple points up to one year post-surgery.
Can estrogen therapy after surgery improve fertility?
Yes. Research shows that women who received estrogen after missed abortion surgery had higher pregnancy rates at one-year follow-up compared to those who received no estrogen, with the strongest outcomes in the transdermal group.
Recommended
- Post-surgical hormonal support: What women need to know | The Asherman’s Compass
- Hysteroscopy for Asherman’s Syndrome: What Nobody Told Me | The Asherman’s Compass
- Can You Get Pregnant With Asherman’s Syndrome? What I Learned | The Asherman’s Compass
- Blog — The Asherman’s Compass
Ready to Understand Your Body Better?
The Complete Asherman's Compass Guide covers everything from diagnosis to recovery — written from lived experience, backed by evidence.
Get the Complete Guide — $97Medical Disclaimer: This article is written from personal experience and is for informational purposes only. It is not medical advice. Please consult a qualified healthcare professional for diagnosis and treatment. The Asherman's Compass does not provide medical diagnoses.
Last reviewed: May 2026