How to Monitor Recovery After Asherman’s Surgery

Surgery for Asherman’s syndrome is a significant step toward reclaiming your uterine health and fertility. But the procedure itself is only half the picture. How you monitor recovery after Asherman’s surgery in the weeks that follow shapes everything: whether adhesions return, whether your lining rebuilds, and whether you catch problems before they become setbacks. Most women leave the operating room without a clear map of what to watch for. This guide gives you that map.
Table of Contents
- Key Takeaways
- What to expect right after surgery
- How to monitor symptoms in the first 6 weeks
- Medical follow-up and imaging after surgery
- Holistic care that supports your recovery
- My honest take on recovery and self-advocacy
- Your recovery does not have to be a guessing game
- FAQ
Key Takeaways
| Point | Details |
|---|---|
| Recovery timeline is 4 to 6 weeks | Most women experience full physical healing within 4 to 6 weeks with proper post-surgery care for Asherman’s. |
| Symptom tracking is non-negotiable | Keeping a daily log of bleeding, pain, and discharge helps you and your doctor catch deviations early. |
| Medical follow-up is time-sensitive | Second-look hysteroscopy at 2 to 3 months post-op confirms uterine restoration and guides next steps. |
| Device removal deadlines matter | The Foley balloon is typically removed around day 7. Missing that window affects your adhesion prevention outcomes. |
| Holistic care accelerates healing | Sleep, nutrition, and emotional support are not optional extras. They directly affect tissue repair and recovery speed. |
What to expect right after surgery
Asherman’s surgery, known as hysteroscopic adhesiolysis, removes scar tissue from inside the uterus using a thin camera inserted through the cervix. There is no incision. Most women are discharged the same day and back home within hours. What you feel in those first days matters, and knowing what is normal stops you from spiraling into worry about symptoms that are completely expected.
Typical recovery involves mild cramping and light bleeding for several days, with full healing expected by 4 to 6 weeks. Acetaminophen or ibuprofen handle the pain effectively for most women. If your pain is escalating after day two rather than settling, that is worth a call to your surgeon.
Your activity and hygiene restrictions are not arbitrary. Avoiding intercourse, tampons, baths, and swimming for approximately two weeks reduces your infection risk and keeps the healing environment inside your uterus stable. This is one of the most overlooked recovery tips after surgery. Breaking these restrictions early is one of the most common ways women unknowingly create complications.
Two medical treatments often accompany the procedure and both require active monitoring on your part:
- Estrogen therapy: Estrogen supports lining regrowth and reduces the likelihood of adhesions returning. Most surgeons prescribe it for 4 to 8 weeks post-op, sometimes combined with progestin.
- Anti-adhesion devices: Balloon catheters or small IUDs are placed inside the uterus immediately after surgery to keep the walls from re-adhering while they heal.
- Antibiotics: A short antibiotic course is standard to prevent post-operative infection.
- Conception timing: Waiting 1 to 3 menstrual cycles before trying to conceive gives your lining time to properly restore.
Pro Tip: Before you leave the hospital, write down the exact name and dose of every medication prescribed, plus the date your balloon catheter or IUD is scheduled for removal. Put a phone alarm on that removal date. You do not want to miss it.
How to monitor symptoms in the first 6 weeks
This is where you become the most important member of your recovery team. Your surgeon sees you for 20 minutes every few weeks. You live in your body 24 hours a day. That gives you information no imaging test can replicate. Here is how to use it.
- Track bleeding daily. Light spotting to a light flow is normal for the first week or two. Write down the color (pink, red, brown) and the volume (spotting, light, moderate). A sudden increase in bright red bleeding after things were settling is a red flag.
- Rate your pain every morning. Use a simple 1 to 10 scale. Mild cramps that fade over the first few days are expected. Pain that increases after day three, radiates into your back or legs, or comes with fever above 100.4°F (38°C) warrants same-day contact with your doctor.
- Note any discharge. Clear or light-colored discharge is normal. Yellow, green, or foul-smelling discharge suggests infection.
- Check your temperature once a day for the first week. A fever is often the first sign of a uterine infection, and catching it early changes your treatment outcome significantly.
- Assess your activity tolerance. Monitoring your ability to perform basic daily activities is a real indicator of healing progression. If you were doing light housework on day five and can barely get off the couch on day eight, something has changed.
- Log your emotional state. This sounds soft but it is practical. Anxiety spikes, mood crashes, and persistent insomnia can all signal that your body is under more stress than expected, or that your hormonal protocol needs adjustment.
A notes app on your phone works perfectly for this. You do not need a specialized tool. What you need is consistency. Even two sentences a day gives your doctor a timeline they would never otherwise have access to. Symptom diary keeping and recognizing deviations from expected patterns is specifically recommended by aftercare specialists.
Pro Tip: Take a photo of your pad or pantiliner once a day in the first week. It sounds strange, but having a visual record of bleeding changes can help you communicate with your doctor far more precisely than trying to describe it from memory.
You can also review this symptom checklist resource from Theashermanscompass to cross-reference what you are tracking against known post-op patterns.
Medical follow-up and imaging after surgery
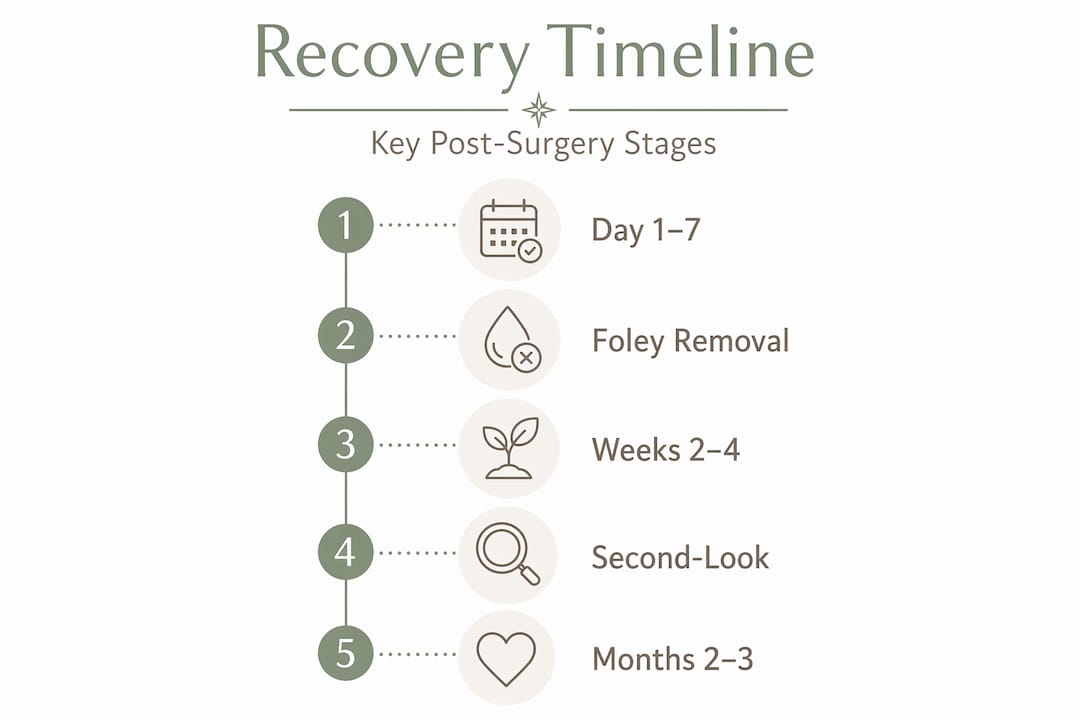
Physical symptoms tell part of the story. Medical imaging and procedures tell the rest. The Asherman’s surgery recovery timeline has specific checkpoints that serve as your formal verification that healing is happening as it should.
![]()
The most critical timeline item for many women is the Foley balloon. This device is typically removed around day 7 post-op, and missing that window is not a minor inconvenience. Leaving it in longer can actually increase irritation and undermine the anti-adhesion benefits it was placed to provide. Confirm this appointment before you leave the hospital.
Here is what the broader Asherman’s surgery follow-up schedule typically looks like:
| Timeframe | What happens | Why it matters |
|---|---|---|
| Day 7 (approx.) | Foley balloon or IUD removal | Prevents device-related irritation and maintains anti-adhesion benefit |
| Weeks 4 to 6 | First post-op appointment | Pain check, infection screen, and review of estrogen therapy response |
| 2 to 3 months post-op | Second-look hysteroscopy | Confirms uterine cavity restoration and checks for adhesion recurrence |
| 3 to 6 months | Ultrasound or further hysteroscopy | Assesses endometrial lining thickness and fertility readiness |
The second-look hysteroscopy is arguably the most important appointment in your Asherman’s syndrome recovery. Hysteroscopy is the gold standard for confirming that your uterine cavity has restored properly. No ultrasound can tell you the same thing with the same precision. Second-look hysteroscopy at 2 to 3 months post-op is standard practice and extends monitoring well beyond when your immediate symptoms resolve.
If you want to understand what that procedure involves in detail before you go, Theashermanscompass has a thorough breakdown of hysteroscopy for Asherman’s that covers what to expect and what to ask.
Women with moderate to severe adhesions face a recurrence risk of up to 20 to 30 percent even after successful surgery. This is not said to alarm you. It is said so you understand why monitoring healing after surgery does not stop when you start feeling better physically. Your follow-up appointments are not formalities. They are how you know.
Holistic care that supports your recovery
The medical protocol covers a lot. What it rarely covers is everything else your body needs to heal well. Post-surgery care for Asherman’s does not live in a prescription bottle alone.
Nutrition for tissue repair is specific, not general. Your uterine lining needs collagen synthesis to rebuild. That means prioritizing protein (eggs, legumes, fish, meat), vitamin C (bell peppers, strawberries, citrus), and zinc (pumpkin seeds, chickpeas, beef). Iron is also worth watching if your bleeding is heavier than expected. A simple blood test can flag deficiency before fatigue becomes a real problem.
Movement is medicine, but only within limits. Light walking from day one or two supports circulation and reduces the risk of blood clots. What you want to avoid in the first two weeks is anything that raises your intra-abdominal pressure: heavy lifting, vigorous exercise, and swimming. After two weeks, your surgeon will guide your return to fuller activity. Mobility and pain management during early recovery are both critical factors in supporting healing progression without triggering complications.
Sleep often gets dismissed as a passive activity. It is not. Tissue repair happens predominantly during deep sleep. Women who sleep under six hours a night during recovery consistently report slower symptom resolution and more fatigue. Prioritize sleep the way you would a medication dose.
- Stress reduction matters more than you think. Elevated cortisol interferes with the hormonal balance your estrogen therapy is trying to create. Even 10 minutes of gentle breathing or body scan meditation daily has a measurable effect on stress hormones.
- Seek community. Recovery from Asherman’s can feel isolating because most people in your life have never heard of it. Online support groups and communities of women who have been through the same surgery provide something clinical care cannot: the specific reassurance of people who actually know what you are going through.
- Consider counseling if you are struggling emotionally. Asherman’s syndrome recovery carries grief, whether over lost pregnancies, fertility uncertainty, or years of dismissed symptoms. A therapist who understands reproductive trauma can be genuinely useful, not just comforting.
For emerging cases where initial surgery has not fully resolved the adhesions, stem cell therapies show significant promise in improving endometrial thickness and pregnancy outcomes. This is worth asking your specialist about if standard protocols are not producing the results expected.
You should also be informed about the hormonal side of your recovery. Theashermanscompass covers post-surgical hormonal support in detail, including what short-term estrogen-progestin therapy actually does and does not do to your body.
Pro Tip: Ask your doctor to check your ferritin level at your first post-op appointment, not just your hemoglobin. Ferritin depletes before anemia shows up on standard tests, and low ferritin is one of the most common reasons women feel exhausted and foggy during recovery.
My honest take on recovery and self-advocacy
I went through this surgery myself, and what I wish someone had told me is this: the medical system gives you a procedure and a prescription. It does not give you a roadmap for the weeks that follow. That gap is not malice. It is just that most surgeons see dozens of patients and assume women will ask if something goes wrong. But many women do not ask. They wait. They assume their symptoms are normal because nobody said they were not.
What I have learned is that the women who recover best are the ones who show up to every follow-up appointment with a written list of questions and a symptom log in hand. Not because they are being difficult. Because that information changes what the doctor does next. I have seen women catch early adhesion recurrence because they noticed their period was lighter than expected at week six and said something. That is not luck. That is monitoring.
I also think the emotional side of Asherman’s recovery is wildly underestimated in clinical care. You are not just healing a uterus. You are often grieving, hoping, and waiting all at once. That is a lot to carry while also trying to rest and recover. If you are struggling emotionally and your surgeon has not mentioned counseling, that is not a sign you are overreacting. That is a gap in your care that you are allowed to fill yourself.
You are not a passive patient in this process. You are the most important variable in your own recovery. The more clearly you can see what is happening in your body, and the more clearly you can communicate it, the better your outcomes will be.
— Daniella
Your recovery does not have to be a guessing game
At Theashermanscompass, we built a recovery guide specifically for women walking this road. The Complete Recovery Guide covers 120 pages of structured, evidence-informed guidance: from what to expect in the first 24 hours to how to prepare for your second-look hysteroscopy, with 18 specialist-ready question scripts and a global directory of Asherman’s specialists. It was written by Daniella, who has lived this experience, not by someone who read about it in a textbook. If you want to understand what you are going through and how to advocate for yourself at every appointment, this is the resource that replaces the scramble. And if you want to know who built it and why, read Daniella’s story before you decide.
FAQ
How long does recovery from Asherman’s surgery take?
Most women experience mild cramping and light bleeding for the first few days, with full physical healing expected by 4 to 6 weeks. Medical monitoring including second-look hysteroscopy typically continues through months 2 to 3.
What symptoms after Asherman’s surgery should concern me?
Contact your doctor promptly if you develop fever above 100.4°F, increasing rather than decreasing pain after day three, heavy bright red bleeding, or foul-smelling discharge. These may indicate infection or other complications.
When is the Foley balloon removed after surgery?
The Foley balloon is typically removed around day 7 post-op. Missing this scheduled removal can increase irritation and reduce the effectiveness of adhesion prevention.
Do I need a second-look hysteroscopy after Asherman’s surgery?
Yes. A second-look hysteroscopy at 2 to 3 months post-op is the standard way to confirm uterine cavity restoration. Ultrasound alone cannot provide the same level of confirmation.
Can adhesions come back after surgery?
Yes, recurrence is possible, particularly in moderate to severe cases. This is exactly why consistent post-op monitoring and timely follow-up appointments are so critical to long-term outcomes.
Recommended
- How to manage pain after Asherman’s procedure | The Asherman’s Compass
- Asherman’s Recovery Tracker — $4.99/month
- Can You Get Pregnant With Asherman’s Syndrome? What I Learned | The Asherman’s Compass
- Post-surgical hormonal support: What women need to know | The Asherman’s Compass
Ready to Understand Your Body Better?
The Complete Asherman's Compass Guide covers everything from diagnosis to recovery — written from lived experience, backed by evidence.
Get the Complete Guide — $97Medical Disclaimer: This article is written from personal experience and is for informational purposes only. It is not medical advice. Please consult a qualified healthcare professional for diagnosis and treatment. The Asherman's Compass does not provide medical diagnoses.
Last reviewed: May 2026