What Cycle Irregularity Diagnosis Actually Involves

If your periods have become unpredictable, lighter, heavier, or nearly absent, you probably want more than a shrug and a prescription for the pill. Understanding what does cycle irregularity diagnosis involve gives you the power to walk into your next appointment knowing what to ask, what to expect, and what the answers actually mean. The formal term clinicians use is abnormal uterine bleeding or menstrual cycle irregularity, and the diagnostic process is more structured than most women are told.
Table of Contents
- Key Takeaways
- What cycle irregularity diagnosis involves: the first clinical steps
- The role of imaging in diagnosing irregular cycles
- Hormonal and specialized lab testing
- Endometriosis and other reproductive health factors
- Interpreting results and planning next steps
- My perspective on getting this right
- How Theashermanscompass can help you move forward
- FAQ
Key Takeaways
| Point | Details |
|---|---|
| Diagnosis follows a structured process | Clinicians use the PALM-COEIN framework to categorize causes as structural or non-structural before ordering tests. |
| Timing matters for hormone tests | Blood draws for FSH, LH, and estrogen must align with your cycle phase to avoid misleading results. |
| Imaging is a first-line tool | Transvaginal ultrasound can identify fibroids, polyps, and endometrial changes before any invasive procedures. |
| Fertility goals shape the process | Reproductive plans directly influence which tests are ordered and which treatment paths are offered. |
| Irregularity is rarely “just hormones” | Gaps over 35 days between periods should be investigated, as underlying causes can affect long-term reproductive health. |
What cycle irregularity diagnosis involves: the first clinical steps
The first thing most clinicians do when you present with irregular cycles is take a thorough history. Not just “how long has this been happening,” but detailed questions about cycle length, flow volume, pain, recent pregnancies, contraception use, and family history of bleeding disorders. This conversation matters more than most patients realize because it shapes every test that follows.
A physical and pelvic exam typically comes next. Your provider checks for signs of structural abnormality, hormonal imbalance, or disease. This is not just routine box-ticking. Findings like an enlarged uterus, tenderness, or skin changes can point directly toward or away from specific diagnoses.
From there, basic laboratory work forms the foundation of the menstrual cycle diagnosis process. The standard initial labs include:
- Complete blood count (CBC): Checks for anemia caused by heavy or prolonged bleeding
- Thyroid function tests: Thyroid disorders are a surprisingly common and easily treated cause of cycle disruption
- Pregnancy test: Ruling out pregnancy first is the clinical priority before any other investigation
- Coagulation profile: Screens for clotting disorders that may explain heavy bleeding
- Prolactin: Elevated levels can suppress ovulation and disrupt cycle regularity
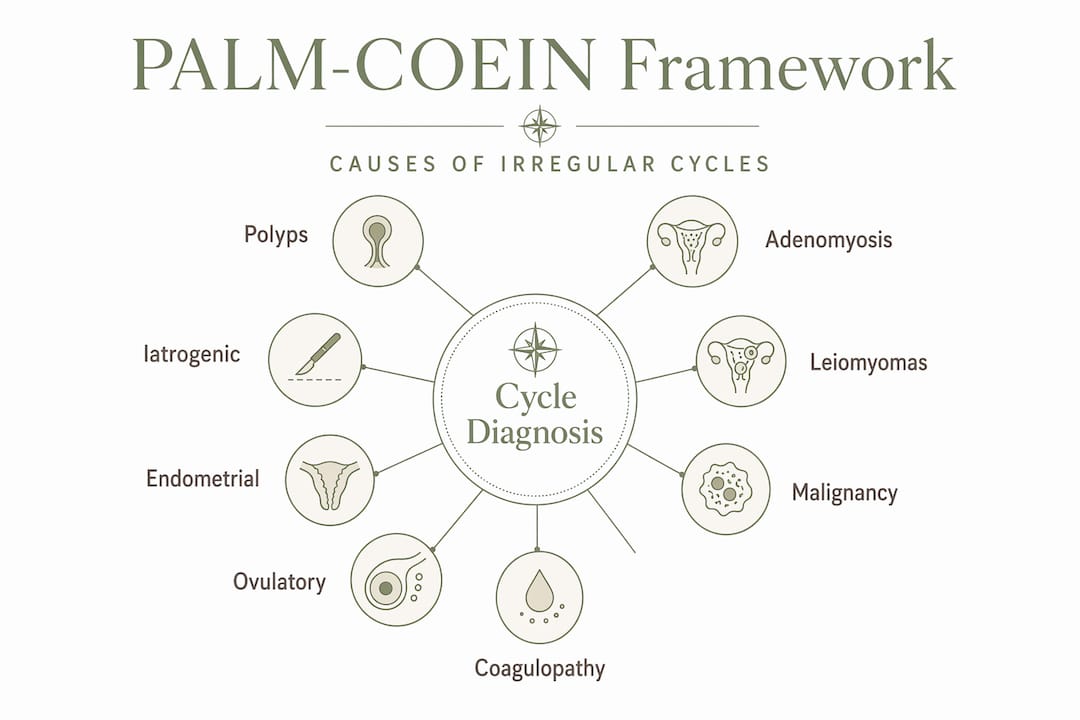
Clinicians use the PALM-COEIN framework to organize findings. PALM covers structural causes like polyps, adenomyosis, leiomyoma (fibroids), and malignancy. COEIN covers non-structural causes including coagulopathy, ovulatory dysfunction, endometrial issues, and iatrogenic causes. This structured differential diagnosis prevents your symptoms from being dismissed as vague hormonal fluctuations.
Pro Tip: Bring a written cycle log to your first appointment. Include cycle length, flow heaviness rated 1 to 10, and any associated symptoms like pain or spotting. Clinicians who see a 6-month pattern make better decisions than those working from memory.
The role of imaging in diagnosing irregular cycles
Imaging is often the step that separates a diagnosis from a guess. Transvaginal ultrasonography is the first-line imaging tool for evaluating the uterus, ovaries, and endometrial lining. It gives your provider a direct look at the internal environment without surgery.

Here is what different imaging findings typically suggest:
| Finding on Imaging | What It May Indicate |
|---|---|
| Thickened endometrial lining | Endometrial hyperplasia, polyp, or hormonal imbalance |
| Submucosal fibroid | Structural cause of heavy or irregular bleeding |
| Ovarian cysts or enlarged ovaries | Polycystic ovary syndrome (PCOS) or other ovarian pathology |
| Diffuse uterine enlargement with thickened walls | Adenomyosis |
| Normal uterus and ovaries | Suggests functional or hormonal cause rather than structural |
When standard ultrasound does not give a clear picture, your provider may recommend advanced imaging. Saline infusion sonography, sometimes called a sonohysterogram, involves injecting saline into the uterine cavity to outline the interior walls. Three-dimensional ultrasound provides detailed architectural views of the uterus and is particularly useful when a congenital abnormality or Asherman’s syndrome is suspected. If you are wondering how Asherman’s is diagnosed, imaging is typically where that investigation begins.
Pro Tip: Ask your provider whether your ultrasound was done vaginally or abdominally. Transvaginal ultrasound is significantly more accurate for evaluating the uterus and endometrial lining. An abdominal scan alone can miss important findings.
Hormonal and specialized lab testing
Once structural causes are assessed, the focus shifts to hormonal and specialized lab work. These tests identify whether ovulatory dysfunction, thyroid disease, or another endocrine condition is driving your irregular cycles.
The core hormone tests used in diagnosing cycle irregularities include:
- FSH and LH: Follicle-stimulating hormone and luteinizing hormone levels reveal how well the brain-ovary communication system is functioning
- Estradiol: Low levels can explain missed periods and affect bone density over time
- Thyroid-stimulating hormone (TSH): Both underactive and overactive thyroid cause cycle disruption
- Prolactin: Even mildly elevated prolactin without a visible pituitary tumor can disrupt ovulation
- Androgens (testosterone, DHEAS): Elevated levels suggest PCOS or adrenal disorders
The timing of these tests is not arbitrary. Cycle-phase dependent testing is critical because FSH and LH levels fluctuate dramatically across the cycle. Drawing blood at the wrong point gives misleading data. Clinicians align lab draws with where you likely are in your cycle, or they interpret results knowing that ovulation status affects everything.
When a woman reports very heavy periods, a detailed bleeding disorder screen is warranted. Von Willebrand disease, the most common inherited bleeding disorder, is frequently underdiagnosed in women because heavy periods are often normalized. If there is a family history of bleeding problems, your provider should ask specifically about this.
A fertility evaluation checklist from a reproductive specialist can be a useful companion to these tests, particularly if you are trying to conceive.
Endometriosis and other reproductive health factors
Endometriosis deserves its own section in the diagnostic conversation because it is both common and commonly missed. Irregular or painful periods are among its signature symptoms, yet the average time to diagnosis remains several years from first symptom onset.
Clinicians evaluate for endometriosis using a combination of approaches:
- Detailed symptom review: Pelvic pain with periods, pain with intercourse, painful bowel movements around menstruation, and infertility are key indicators
- Pelvic examination: Tenderness, nodules on the uterosacral ligaments, or a fixed uterus suggest disease
- Transvaginal ultrasound: Identifies ovarian endometriomas (chocolate cysts) but may miss superficial peritoneal deposits
- MRI: Provides better detail for deep infiltrating endometriosis
- Surgical diagnosis: ACOG guidelines confirm that surgical evaluation, typically laparoscopy, may be required when imaging and clinical signs are inconclusive
The intersection between endometriosis and fertility is significant. Research on endometriosis and uterine scarring shows how these two conditions can compound each other, creating a more complex fertility picture that requires careful evaluation.
| Diagnostic approach | Best suited for |
|---|---|
| Clinical evaluation alone | Mild symptoms with clear hormonal pattern |
| Ultrasound plus labs | Suspected structural cause or PCOS |
| MRI | Suspected deep infiltrating endometriosis |
| Laparoscopy | Inconclusive imaging with persistent symptoms or infertility |
When reproductive goals are part of the picture, the diagnostic strategy shifts. Cycle irregularities with fertility concerns require an integrated evaluation of ovulatory function and the endometrial environment together, not as separate investigations. Your reproductive goals are not a footnote. They should be part of the first conversation.
Interpreting results and planning next steps
Getting results back is one thing. Understanding what they mean for your life is another. Once the diagnostic picture is clearer, causes generally fall into four categories: structural, hormonal, bleeding-related, or a combination. This categorization directly shapes the treatment options your provider offers.
Heavy bleeding soaking through one or more pads per hour for more than four hours requires urgent evaluation. That is not a “watch and wait” situation. Most other findings, including oligomenorrhea with cycles longer than 35 days, are managed in an outpatient setting but still need timely investigation because underlying causes can affect long-term reproductive health.
Treatment options for cycle irregularity range from hormonal therapy and targeted medication to surgical intervention, depending on the cause. A fibroid causing heavy bleeding is managed differently from a thyroid condition disrupting ovulation. This is why the diagnostic process exists: to match the treatment to the actual problem rather than applying a one-size approach.
Pro Tip: After receiving results, ask your provider to classify your diagnosis using the PALM-COEIN categories. It sounds technical, but understanding whether your issue is structural or functional changes which questions you ask next and which specialists you may need.
If symptoms like cramping persist without a clear flow, that warrants specific investigation. You can read more about what cramping without bleeding may signal for women with a history of uterine procedures.
My perspective on getting this right
I spent years being told my cycles were “probably just stress.” After Asherman’s, after multiple losses, I know exactly what it feels like to leave a doctor’s office with a reassurance that explains nothing.
What I’ve learned is that the women who get answers fastest are the ones who come in prepared. Not aggressive, not demanding. Just informed. When you understand that PALM-COEIN is a real clinical framework and not something you read on a forum, doctors treat your concerns differently. They hear that you understand the process, and they stop defaulting to the dismissal script.
I’ve also seen, repeatedly, that irregular cycles are not a single problem. They are a symptom pointing toward something else. The diagnostic steps I’ve described above are not bureaucratic hoops. They are the actual path from “something is wrong” to “here is what it is and here is what we can do.” Every woman deserves that path to be walked properly, not shortcut.
The uncomfortable truth is that many of us have to advocate for the thorough evaluation described here. Know what questions to ask. Know what tests should be offered. And if a provider dismisses gaps longer than 35 days as normal, know that the clinical evidence says otherwise.
— Daniella
How Theashermanscompass can help you move forward
If you are in the middle of this diagnostic process and feeling overwhelmed, you are not alone. Theashermanscompass was built precisely for this moment.
The Complete Recovery Guide walks you through the entire diagnostic and recovery process in plain language, including 18 specialist-ready question scripts you can bring to any appointment. Whether you are dealing with light periods, missing periods, post-procedure changes, or unexplained cycle disruption, the guide gives you a clear roadmap. If you are not sure where you stand yet, start with the free symptom quiz to help identify what might be driving your symptoms. Because you deserve answers, not another referral and a shrug.
FAQ
What does a cycle irregularity diagnosis start with?
Diagnosis begins with a detailed clinical history, pelvic exam, and basic labs including a pregnancy test, CBC, thyroid function, and coagulation profile, organized around the PALM-COEIN framework.
How long should a menstrual cycle be?
A normal cycle runs between 21 and 35 days. Cycles consistently shorter or longer than this range, or fewer than six to eight periods per year, qualify as irregular and warrant evaluation.
What hormone tests are used for irregular cycles?
Clinicians typically test FSH, LH, estradiol, prolactin, thyroid-stimulating hormone, and sometimes androgens. The timing of these tests relative to your cycle phase directly affects the accuracy of results.
Can endometriosis cause cycle irregularities?
Yes. Endometriosis can cause painful, irregular, or heavy periods. Diagnosis involves clinical assessment, ultrasound, and sometimes laparoscopy when imaging findings are inconclusive per ACOG guidelines.
When should irregular bleeding be treated urgently?
Bleeding that soaks through one or more pads per hour for more than four hours requires urgent medical evaluation, as does any postmenopausal bleeding or bleeding between periods with significant pain.
Recommended
- How Is Asherman’s Syndrome Diagnosed? | The Asherman’s Compass
- Unexplained Infertility: Could Uterine Scarring Be the Answer? | The Asherman’s Compass
- Period Cramps But No Flow: Could It Be Asherman’s Syndrome? | The Asherman’s Compass
- Thin Uterine Lining: Causes, Symptoms & What Actually Helps | The Asherman’s Compass
Ready to Understand Your Body Better?
The Complete Asherman's Compass Guide covers everything from diagnosis to recovery — written from lived experience, backed by evidence.
Get the Complete Guide — $97Medical Disclaimer: This article is written from personal experience and is for informational purposes only. It is not medical advice. Please consult a qualified healthcare professional for diagnosis and treatment. The Asherman's Compass does not provide medical diagnoses.
Last reviewed: May 2026