Diagnostic Delay in Women: What You Need to Know

If you’ve spent months or years being told your symptoms are normal, your pain is stress, or your miscarriages are “just bad luck,” you’ve already lived what researchers call a diagnostic delay. What is diagnostic delay women explained simply: it’s the gap between when your symptoms begin and when you receive an accurate diagnosis. For women with conditions like Asherman’s syndrome, unexplained infertility, and recurrent miscarriage, that gap can stretch for years. It shapes your treatment options, your fertility outcomes, and your mental health in ways that are rarely acknowledged. This article breaks down why it happens, what it costs you, and what you can do about it today.
Table of Contents
- Key takeaways
- What is diagnostic delay in women explained
- Condition-specific delays you should know about
- The real cost of waiting too long
- How to shorten your own diagnostic delay
- My honest take on why this keeps happening
- Your next step starts here
- FAQ
Key takeaways
| Point | Details |
|---|---|
| Diagnostic delay is systemic | Delays are rooted in medical bias, not just individual doctor failures, affecting millions of women globally. |
| Conditions most affected | Asherman’s syndrome, endometriosis, unexplained infertility, and recurrent miscarriage carry the longest average delays. |
| Earlier evaluation is standard | Full evaluation after two pregnancy losses is now recommended, especially for women over 35. |
| Delays worsen outcomes | The longer a condition goes undiagnosed, the greater the impact on fertility, symptoms, and emotional health. |
| Self-advocacy changes outcomes | Documenting symptoms, asking targeted questions, and seeking specialist referrals can meaningfully shorten your delay. |
What is diagnostic delay in women explained
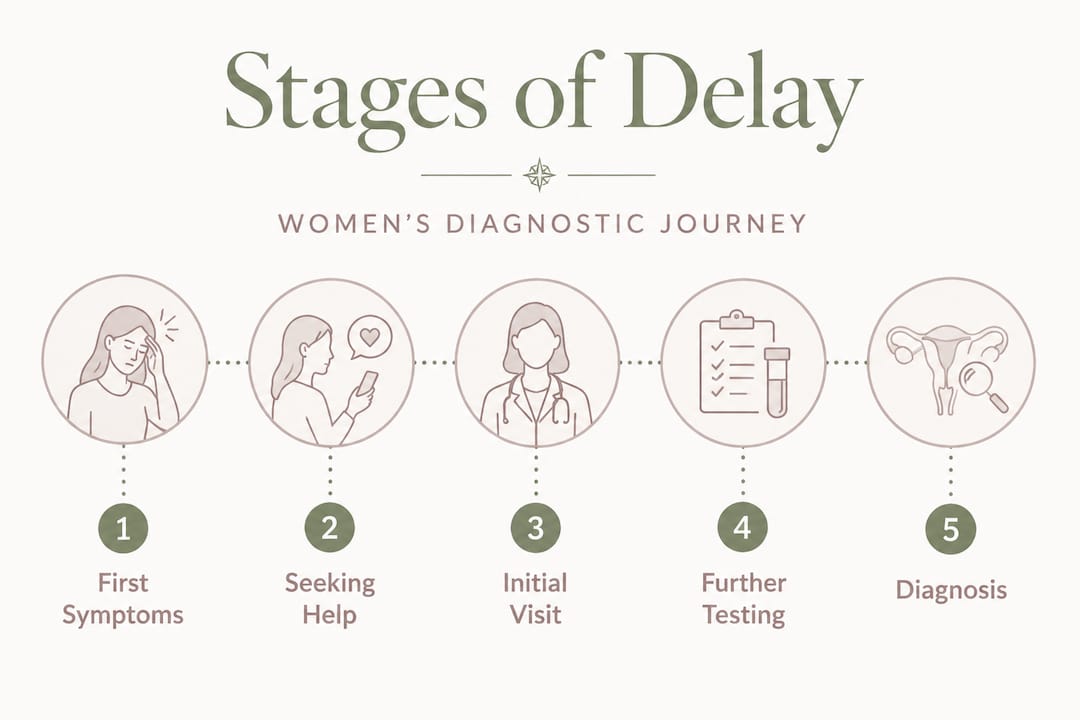
Diagnostic delay in women refers to the time between when symptoms first appear and when a correct diagnosis is made. This sounds straightforward, but in practice it involves multiple layers: the time before a woman seeks care, the time spent being dismissed or misdiagnosed, and the time waiting for the right specialist or test. Each layer adds weeks, months, or years to the clock.
Women experience longer delays than men across many diseases because their symptoms are often atypical, less studied, or filtered through assumptions about pain tolerance and emotional sensitivity. The medical system was built on research that historically excluded women, which means diagnostic criteria for many conditions were developed without a full picture of how those conditions actually present in female bodies.
The causes of diagnostic delay are not random. They fall into three broad categories. First, systemic bias: a medical culture that has long normalized women’s pain and treated it as a psychological rather than physiological issue. Second, knowledge gaps: many providers are simply not trained to recognize conditions like Asherman’s syndrome or to connect light periods after a D&C to uterine scarring. Third, structural barriers: long wait times for specialists, limited access to gold-standard diagnostic tools, and a referral system that keeps many women in generalist care longer than necessary.
Pro Tip: If a provider tells you your symptoms are “normal” without ordering any tests, that is a signal to ask specifically which test would rule out the conditions you’re concerned about. Make them name it.
Understanding diagnostic delay in healthcare means recognizing that the problem is not just one bad appointment. It’s a pattern, and patterns can be interrupted.
Condition-specific delays you should know about
Some conditions carry notoriously long diagnostic timelines. Knowing the averages gives you a benchmark to measure your own experience against.
| Condition | Average Diagnostic Delay | Key Diagnostic Tool | Common Barrier |
|---|---|---|---|
| Endometriosis | 7 to 12 years | Laparoscopy | Symptom normalization |
| Asherman’s syndrome | Months to years post-procedure | Hysteroscopy | Generalist referral gaps |
| Unexplained infertility | 12 months trying (6 months if 35+) | Exclusion of known causes | No clear diagnostic marker |
| Recurrent miscarriage | After 2 consecutive losses | Genetic, hormonal, uterine imaging | Outdated “wait for three” approach |
Endometriosis is the most documented example of diagnostic delay in women’s reproductive health. Despite affecting 10 to 15% of reproductive-age women, the average delay from symptom onset to diagnosis remains stubbornly long. Critically, delays have not significantly improved in 20 years, even as public awareness has grown. That gap between awareness and actual clinical practice is where most women get lost.

Asherman’s syndrome presents a different kind of delay. Most women don’t know it exists until they’re already searching for answers about light periods, absent periods, or failed IVF cycles after a uterine procedure. General OB/GYNs typically don’t perform hysteroscopy, which is the gold-standard diagnostic tool, so women often spend months in the wrong clinical setting before reaching a reproductive specialist who can actually see what’s happening inside the uterus. You can read more about how Asherman’s is diagnosed and what to expect from that process.
For unexplained infertility, the definition itself creates a built-in delay. Diagnosis requires 12 months of trying with normal standard fertility tests, or 6 months if you’re 35 or older. That timeline is clinically appropriate, but it can feel like a waiting game with no clear endpoint. The good news: 60 to 70% of couples with unexplained infertility achieve live births through structured treatment, which means no diagnosis does not mean no path forward. If you suspect uterine scarring may be behind an unexplained infertility label, uterine scarring as a cause is worth exploring with your provider.
Recurrent miscarriage evaluation has also shifted. The outdated standard of waiting for three losses before investigating is no longer supported by current clinical guidance. Full evaluation after two consecutive losses is now recommended, particularly for women over 35. This matters because each additional loss without investigation is not just emotionally devastating. It’s a missed opportunity to find a treatable cause.
The real cost of waiting too long
Diagnostic delays don’t just delay treatment. They actively worsen outcomes. This is one of the most under-discussed aspects of understanding diagnostic delay in healthcare.
For conditions like endometriosis, delayed diagnosis means more time for lesions to progress, more damage to surrounding tissue, and a more complex surgical picture when treatment finally begins. For Asherman’s syndrome, scar tissue can thicken and spread within the uterine cavity the longer it goes untreated, reducing the chances of successful adhesiolysis. For recurrent miscarriage, each additional loss without evaluation increases the cumulative emotional toll and, in some cases, the likelihood of identifying a cause that could have been treated earlier.
The emotional impact of diagnostic delay in women is significant and well-documented. Women describe years of being told they are anxious, dramatic, or simply unlucky. That experience doesn’t disappear when a diagnosis finally arrives. It shapes how women interact with the medical system afterward, often making them less likely to advocate for themselves and more likely to accept inadequate explanations.
“The delay wasn’t just in my diagnosis. It was in being believed. And that second delay is the one that took the longest to recover from.”
The long-term quality-of-life implications extend beyond fertility. Chronic pain, repeated pregnancy loss, and years of unexplained symptoms affect relationships, careers, mental health, and self-perception. The impact of diagnostic delay is not a footnote. It’s the whole story for many women.
How to shorten your own diagnostic delay
You cannot fix the medical system by yourself. But you can change how you move through it. Here’s what actually works.
-
Document everything in writing. Date your symptoms, describe them specifically, and note how they relate to your cycle. Detailed records of losses and symptoms are one of the most effective ways to trigger appropriate clinical evaluation early. Providers respond differently to a written timeline than to a verbal summary.
-
Know the diagnostic tools for your suspected condition. For Asherman’s syndrome, that means hysteroscopy, not just ultrasound. For endometriosis, it means laparoscopy, not just a pelvic exam. Asking your provider specifically whether they can perform or refer you for the gold-standard test puts the conversation on clinical ground rather than symptomatic ground.
-
Request a specialist referral sooner than feels comfortable. Most women wait too long to ask for a referral because they don’t want to seem demanding. Asking for a referral to a reproductive endocrinologist or a specialist in uterine conditions is not demanding. It’s appropriate care-seeking. A fertility evaluation checklist can help you understand what tests and benchmarks to expect at each stage.
-
Ask about evaluation timelines explicitly. If a provider recommends waiting, ask: “What is the specific timeline for this approach, and at what point would you recommend moving to the next step?” Expectant management without a defined endpoint is one of the most common ways delays get extended without anyone noticing.
-
Seek a second opinion if your symptoms are dismissed without investigation. This is not disloyal. It’s your right. Women who advocate for second opinions consistently report shorter diagnostic timelines.
Pro Tip: Before any appointment, write down your three most specific, concrete symptoms and the one question you most need answered. Providers respond to specificity. “I’ve had absent periods since my D&C eight months ago” gets a different response than “my periods have been off.”
A framework for knowing when to push harder
If you’ve had two or more pregnancy losses, ask for full evaluation now, not after a third. If your periods changed significantly after a uterine procedure, ask specifically about Asherman’s syndrome and hysteroscopy. If you’ve been trying for 12 months (or 6 months at 35+) with no explanation, ask what comes next and get a timeline in writing. The women who shorten their diagnostic delays are almost always the ones who ask the next question rather than accepting “let’s wait and see” without a defined end date.
My honest take on why this keeps happening
I’ve spent years inside this experience, first as a patient and then as someone who talks to hundreds of women navigating the same maze. The thing that strikes me most is not that individual doctors are cruel or careless. Most aren’t. What I’ve found is that the system rewards patience in patients and punishes urgency. Women who push back are labeled difficult. Women who accept vague reassurances get sent home.
What I’ve learned is that diagnostic delay persists not because we lack the tools to diagnose these conditions. We have hysteroscopy, laparoscopy, genetic testing, hormonal panels. We have all of it. The delay persists because the default assumption is still that a woman’s reproductive symptoms are probably not serious until proven otherwise. That assumption has to be challenged every single time, by you, in the appointment room.
The contrarian view I’d offer is this: “expectant management” without a hard timeline is not a treatment plan. It’s a delay with a clinical name. If your provider recommends waiting, you are entitled to know exactly how long, what they’re watching for, and what happens if nothing changes. Vague waiting is where years disappear.
You are the most important variable in shortening your own diagnostic delay. Not because the burden should be on you. It shouldn’t. But because right now, in this system, your voice in the room is the fastest lever you have.
— Daniella
Your next step starts here
If this article gave you language for something you’ve been living without a name for, that’s exactly what Theashermanscompass was built for. Daniella created it after years of piecing together her own diagnosis from Reddit threads and medical journals at 3am, because no single resource existed that spoke plainly to women in this situation.
The Complete Recovery Guide at Theashermanscompass covers Asherman’s syndrome, recurrent miscarriage, unexplained infertility, and post-procedure complications across 120 pages, 10 chapters, and 18 specialist-ready question scripts. It includes a global specialist directory and a self-care protocol written by someone who walked this path first. If you’re not ready for the full guide, the free Starter Kit gives you symptoms, questions to ask, and where to begin. Either way, you don’t have to piece this together alone.
FAQ
What is a diagnostic delay in women’s health?
A diagnostic delay is the gap between when a woman’s symptoms begin and when she receives an accurate diagnosis. In reproductive health, this gap commonly affects conditions like endometriosis, Asherman’s syndrome, and recurrent miscarriage, often spanning months to years.
How long is the average diagnostic delay for endometriosis?
Women with endometriosis face an average diagnostic delay of 7 to 12 years from symptom onset, with global figures ranging from 4 to 11 years depending on the region and healthcare system.
When should recurrent miscarriage be evaluated?
Current clinical guidance recommends full evaluation after two consecutive pregnancy losses, not three. For women over 35, evaluation after two losses is especially important given the impact of age on fertility outcomes.
Why is Asherman’s syndrome so often missed?
Asherman’s syndrome requires hysteroscopy for accurate diagnosis, a procedure most general OB/GYNs don’t perform. Women often remain in generalist care for months before receiving a referral to a reproductive specialist who can perform the appropriate diagnostic procedure.
Can unexplained infertility still be treated effectively?
Yes. An unexplained infertility label means standard tests found no identifiable cause, not that treatment is impossible. Structured treatment approaches including IVF result in live births for 60 to 70% of couples, making timely progression through treatment stages critical.
Recommended
- Unexplained Infertility: Could Uterine Scarring Be the Answer? | The Asherman’s Compass
- How Is Asherman’s Syndrome Diagnosed? | The Asherman’s Compass
- Period Cramps But No Flow: Could It Be Asherman’s Syndrome? | The Asherman’s Compass
- Endometriosis & Uterine Scarring: How They Affect Fertility Together | The Asherman’s Compass
Ready to Understand Your Body Better?
The Complete Asherman's Compass Guide covers everything from diagnosis to recovery — written from lived experience, backed by evidence.
Get the Complete Guide — $97Medical Disclaimer: This article is written from personal experience and is for informational purposes only. It is not medical advice. Please consult a qualified healthcare professional for diagnosis and treatment. The Asherman's Compass does not provide medical diagnoses.
Last reviewed: May 2026