Symptoms Pointing to Asherman’s Syndrome: Know the Signs

Your periods suddenly got lighter after a D&C. Or they stopped altogether. Maybe you’ve had two miscarriages in a row and nobody can explain why. If any of this sounds familiar, you may already be searching for answers around symptoms pointing to Asherman’s syndrome, a condition where scar tissue forms inside the uterus and quietly disrupts your menstrual cycle, fertility, and overall reproductive health. Asherman’s affects about 1.5% of women of reproductive age, yet it remains one of the most underdiagnosed conditions in gynecology. This guide breaks down exactly what to look for, what gets confused with it, and what to do next.
Table of Contents
- Key Takeaways
- Symptoms pointing to Asherman’s syndrome and how they show up
- Conditions that look like Asherman’s syndrome
- Getting an Asherman’s syndrome diagnosis
- Advocating for yourself when symptoms get dismissed
- What happens after diagnosis
- My honest take after years in this space
- Your next step starts here
- FAQ
Key Takeaways
| Point | Details |
|---|---|
| Symptom timing matters | Menstrual changes that begin after a uterine procedure are a major red flag for Asherman’s syndrome. |
| Pain without bleeding is telling | Severe cramping around your expected period with no blood can mean trapped menstrual flow from scar tissue. |
| Ultrasound often misses it | A normal ultrasound does not rule out Asherman’s. Hysteroscopy is the only reliable diagnostic tool. |
| Misdiagnosis is common | Hormonal imbalances and stress are frequently blamed when Asherman’s is the real cause. |
| Advocacy changes outcomes | Documenting your symptom timeline and requesting specialist referrals can significantly speed up diagnosis. |
Symptoms pointing to Asherman’s syndrome and how they show up
Asherman’s syndrome does not announce itself loudly. For most women, the signs are gradual and easy to explain away, at least at first. Understanding the specific pattern of symptoms is what separates a delayed diagnosis from an early one.
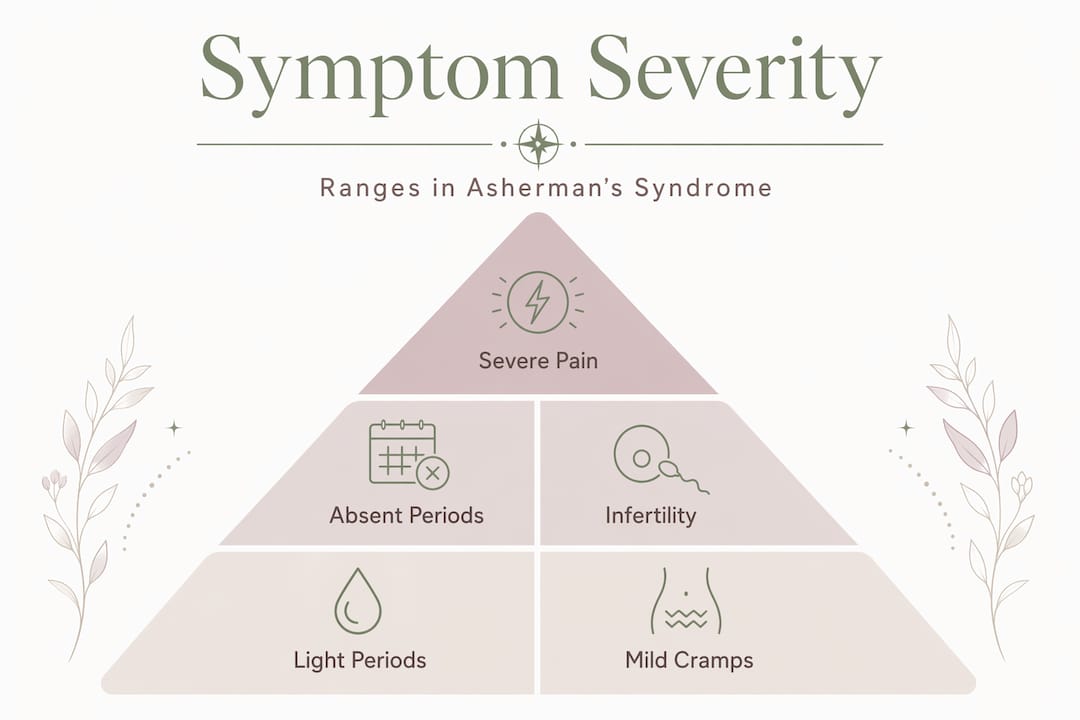
The most recognized signs of Asherman’s syndrome fall into three categories: menstrual changes, pain, and fertility problems. According to clinical data, primary symptoms include hypomenorrhea (very light periods), amenorrhea (absent periods following a uterine procedure), recurrent miscarriage, infertility, and pelvic pain or cramping without any bleeding.
Here is what each of those actually looks like in real life:
- Hypomenorrhea: Your period used to be regular and moderate. After a D&C or uterine surgery, it becomes noticeably lighter. You might go from using several pads or tampons a day to barely spotting.
- Amenorrhea: Your period disappears entirely after a procedure. This is not the same as stress-related missed periods. It is consistent, cycle after cycle, with no hormonal explanation.
- Pelvic pain without bleeding: This one surprises people. Severe cramping occurs around the time your period should arrive, but nothing comes out. Scar tissue can physically block menstrual blood from exiting the uterus, causing it to pool internally.
- Recurrent miscarriage: If you have experienced two or more pregnancy losses and no cause has been found, uterine adhesions may be a factor. Scar tissue reduces the surface area available for implantation.
- Infertility and implantation failure: Repeated failed IVF cycles or an inability to conceive despite normal ovarian function can point toward a uterine issue. Asherman’s reduces pregnancy rates by approximately 70% due to intrauterine fibrosis.
Symptom severity varies depending on how much of the uterine cavity is affected. Mild adhesions might only cause lighter periods. Severe scarring can cause complete amenorrhea and significant pain.
Pro Tip: Keep a period log from the moment something feels “off.” Note flow volume, cycle length, pain levels, and any procedures you have had. This timeline becomes one of your most useful tools when talking to a specialist.
Conditions that look like Asherman’s syndrome
One of the most frustrating parts of this condition is how often it gets misread. Misdiagnosis is common, with hormonal treatments frequently prescribed when the real issue is structural, not hormonal.
These are the conditions most often confused with Asherman’s syndrome:
- Hormonal imbalances: Low estrogen, thyroid dysfunction, and polycystic ovary syndrome (PCOS) all cause irregular or absent periods. The key difference is that hormonal causes typically develop gradually and are not linked to a specific uterine procedure. Asherman’s symptoms tend to appear suddenly after a D&C, hysteroscopy, or cesarean section.
- Endometriosis: Pelvic pain and fertility struggles overlap significantly with Asherman’s. But endometriosis pain usually worsens during menstruation, while Asherman’s pain often occurs instead of menstruation. The flow pattern is different too. Endometriosis rarely causes lighter periods.
- Stress-related menstrual changes: Stress can delay or suppress ovulation, causing irregular cycles. But stress does not cause a sudden, persistent reduction in flow volume that begins the month after a uterine procedure.
- Premature ovarian insufficiency (POI): Elevated FSH levels and low estrogen can mimic Asherman’s amenorrhea. Bloodwork can help distinguish between the two, though some women have both conditions simultaneously.
The clearest differentiator for Asherman’s is timing. Sudden menstrual changes after a D&C are a red flag that demands investigation, even when an ultrasound comes back normal.
Pro Tip: Before your next appointment, write down every uterine procedure you have ever had, including D&Cs, hysteroscopies, cesarean sections, and fibroid removals. Then note when your symptoms started relative to each procedure. That timeline tells the story your bloodwork cannot.
Getting an Asherman’s syndrome diagnosis
Knowing what tests to ask for is half the battle. Many women spend months in a diagnostic loop because the right tool was never used.
Here is how the diagnostic process typically unfolds:
- Medical history review: A good specialist will ask about prior uterine procedures, pregnancy history, and the exact nature of your menstrual changes. This conversation alone can raise or lower suspicion significantly.
- Ultrasound: A standard transvaginal ultrasound is often the first test ordered, but it has real limitations. Ultrasounds frequently miss uterine adhesions because scar tissue does not always appear on standard imaging.
- Saline sonogram (SIS): Saline is injected into the uterus before an ultrasound to improve visualization of the uterine cavity. This is more useful than a standard ultrasound for spotting irregularities.
- Hysterosalpingogram (HSG): Dye is injected through the cervix and X-rays are taken. It can reveal filling defects inside the uterus, which may indicate adhesions. Useful but not definitive.
- Hysteroscopy: This is the gold standard for diagnosis. A thin camera is inserted directly into the uterine cavity, allowing the doctor to see adhesions clearly. It is also therapeutic. Adhesions can be removed during the same procedure.
For more detail on how each of these tools works in practice, the Asherman’s diagnosis guide at Theashermanscompass walks through each step clearly.
| Diagnostic method | Pros | Cons |
|---|---|---|
| Transvaginal ultrasound | Non-invasive, widely available | Often misses adhesions |
| Saline sonogram (SIS) | Better uterine cavity view | Mild discomfort, not always available |
| HSG | Shows uterine shape and tube patency | Radiation exposure, not definitive |
| Hysteroscopy | Direct visualization, can treat simultaneously | Requires specialist, more invasive |
The takeaway here is straightforward. If your symptoms strongly suggest Asherman’s and your ultrasound is normal, push for a hysteroscopy. A normal ultrasound is not a green light. It is just one data point.
Advocating for yourself when symptoms get dismissed
This is where many women lose months, sometimes years. Asherman’s syndrome symptoms are frequently minimized, and the standard response from a generalist gynecologist is often a prescription for hormonal therapy.
Hormonal treatments alone do not address structural scar tissue. If your periods are light or absent because adhesions are physically blocking your uterine cavity, no amount of estrogen will fix that. The structure needs to be addressed directly.
Red flags that mean you should seek a specialist rather than wait:
- Periods that became significantly lighter or stopped after any uterine procedure
- Cramping at period time with no or minimal bleeding
- Two or more unexplained miscarriages
- Failed IVF cycles with no clear explanation
- A doctor who attributes your symptoms entirely to stress or hormones without investigating the uterus
Pro Tip: Before any appointment, prepare a written symptom timeline and a short list of questions. Ask specifically: “Could this be a structural uterine issue?” and “Should I have a hysteroscopy?” Writing it down means you will not forget it in the moment.
When seeking a second opinion, look for a gynecologist who specializes in minimally invasive gynecologic surgery or reproductive surgery. General OBGYNs are not always trained in hysteroscopic adhesiolysis. You can also use this fertility evaluation checklist to understand what a thorough reproductive workup should include before your appointment.
What happens after diagnosis
Getting a confirmed Asherman’s diagnosis is not the end of the road. For most women, it is actually the beginning of a clearer path forward.
The primary treatment is hysteroscopic adhesiolysis, where a surgeon removes the scar tissue directly through the hysteroscope. This procedure is both diagnostic and therapeutic, but outcomes depend heavily on the surgeon’s experience with uterine adhesions. Mild to moderate cases often see significant improvement in menstrual flow and fertility after one procedure. Severe cases may require multiple surgeries.
After surgery, many specialists prescribe estrogen therapy to encourage the uterine lining to regenerate. A follow-up hysteroscopy is often performed to check for recurrence. Uterine factors account for 10 to 15% of female infertility cases, and treating Asherman’s specifically can meaningfully improve pregnancy outcomes for women who want to conceive.
Emerging research into stem cell therapies and regenerative approaches offers hope for women with severe or recurring adhesions, though these are not yet widely available. The most important thing right now is consistent follow-up, tracking your symptoms post-treatment, and staying connected with a specialist who knows this condition well.
My honest take after years in this space
I spent a long time thinking something was wrong with me in a way that could not be named. My periods changed, my doctors shrugged, and I left appointments feeling more confused than when I walked in. What I know now is that the confusion was not a reflection of my body being mysterious. It was a reflection of how poorly this condition is understood at the generalist level.
The women I hear from most often are not lacking medical care. They are lacking the right medical care. They have had ultrasounds that came back normal. They have been told their light periods are “just stress.” They have been prescribed birth control to regulate cycles that were never hormonal to begin with. The delay is not their fault. It is a systemic gap.
What actually moves the needle is this: knowing your own symptom history better than any doctor in the room, asking for the specific tests by name, and refusing to accept “everything looks fine” when your body is telling you otherwise. If you want to understand what a thorough symptom checklist looks like, or you want to take the free symptom quiz to get a clearer picture before your next appointment, both are worth your time.
You are not overreacting. You are paying attention.
— Daniella
Your next step starts here
If this article has you wondering whether your symptoms fit the picture, you do not have to keep piecing it together alone.
Theashermanscompass was built specifically for this moment. The Complete Recovery Guide covers everything from symptom recognition to specialist-ready question scripts, a global directory of Asherman’s specialists, and a full self-care protocol. It is 120 pages of the information that took Daniella years to gather, organized so you can use it on diagnosis day. Whether you are still searching for answers or you have just received a confirmed diagnosis, the Compass gives you a clear, calm roadmap when everything else feels uncertain. And 10% of every sale goes directly to the Compass Fund, which supports specialist care for women who need it most.
FAQ
What are the most common symptoms of Asherman’s syndrome?
The most common symptoms include very light or absent periods after a uterine procedure, severe cramping around the time of an expected period with no bleeding, recurrent miscarriage, and unexplained infertility. Symptoms vary depending on how much scar tissue is present.
Can a normal ultrasound rule out Asherman’s syndrome?
No. Ultrasounds frequently miss intrauterine adhesions. Hysteroscopy is the gold standard diagnostic tool because it allows direct visualization of the uterine cavity and can confirm or rule out scar tissue.
What causes Asherman’s syndrome?
Asherman’s syndrome is most commonly caused by uterine procedures such as dilation and curettage (D&C), hysteroscopy, cesarean section, or fibroid removal. The trauma to the uterine lining triggers scar tissue formation in some women.
How is Asherman’s syndrome treated?
The primary treatment is hysteroscopic adhesiolysis, where a surgeon removes scar tissue directly through a hysteroscope. Mild cases may resolve after one procedure. Severe cases can require multiple surgeries and follow-up monitoring.
Can you get pregnant after Asherman’s syndrome treatment?
Yes, pregnancy is possible after treatment, particularly for women with mild to moderate adhesions. However, Asherman’s syndrome reduces pregnancy rates significantly without treatment, so early diagnosis and intervention matter greatly for fertility outcomes.
Recommended
- Asherman’s Syndrome Symptoms: A Complete Checklist | The Asherman’s Compass
- Could You Have Asherman’s Syndrome? — Free Symptom Quiz
- How Is Asherman’s Syndrome Diagnosed? | The Asherman’s Compass
- Why Are My Periods So Light After a D&C? — The Asherman’s Compass
Ready to Understand Your Body Better?
The Complete Asherman's Compass Guide covers everything from diagnosis to recovery — written from lived experience, backed by evidence.
Get the Complete Guide — $97Medical Disclaimer: This article is written from personal experience and is for informational purposes only. It is not medical advice. Please consult a qualified healthcare professional for diagnosis and treatment. The Asherman's Compass does not provide medical diagnoses.
Last reviewed: May 2026